

NCBI Bookshelf. A service of the National Library of Medicine, National Institutes of Health.
Peterson BS, Trampush J, Maglione M, et al. ADHD Diagnosis and Treatment in Children and Adolescents [Internet]. Rockville (MD): Agency for Healthcare Research and Quality (US); 2024 Mar. (Comparative Effectiveness Review, No. 267.)
6.1. Key Question (KQ) 3 ADHD Monitoring Key Points
- Very few monitoring studies have been reported and more research is needed on how youth with attention deficit hyperactivity disorder (ADHD) should be monitored over time.
- Different assessment modalities may provide valid but different perspectives and more than a single assessment modality may be required for comprehensive and effective monitoring of ADHD outcomes over time.
6.2. KQ 3 ADHD Monitoring Summary of Findings
We identified a small number of studies addressing a monitoring strategy.173, 203, 255, 256, 268, 274, 466, 545, 609, 629 Results of the individual studies are shown in Appendix D, Table D.3. However, studies did not provide information on the predefined key outcomes.
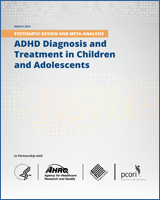
The potential for risk of bias in the KQ3 studies is documented in Figure 92. The critical appraisal for the individual studies is in Appendix D.
Figure 92
Risk of bias in Key Question 3 ADHD monitoring studies. Notes: ADHD = attention deficit hyperactivity disorder
Across studies, selection bias was likely present in two studies.274, 466 Performance bias was present in two studies.268, 274 Attrition bias was also present in two of the identified studies.173, 203 Detection bias was determined to be present in three studies.173, 274, 466 Reporting bias was likely in one study.545 In the small set of studies, a third were rated as high risk of bias for other sources.255, 268, 629
Figure 93 shows the distribution of applicability issues in KQ3 studies. The applicability for the individual studies is in Appendix D.
Figure 93
KQ3 applicability rating. Notes: KQ = Key Question, N/A = not available
Given the small number of available studies, results of the different monitoring strategies are documented in Table 26. More details can be found in Appendix Table C.3.
Table 26
KQ3 monitoring strategies evidence.
We identified 10 studies addressing some type of monitoring strategy for ADHD.173, 203, 255, 256, 268, 274, 466, 545, 609, 629 Three studies of ADHD rating scales and/or a computerized continuous performance task assessed their reliability and sensitivity to detect symptom change over time. The studies reported a relatively poor correlation between these measures over time, whether the correlations were between different raters on the same rating scale545 or between assessment modalities (e.g., rating scale vs computerized performance test).173, 203 Both subjective assessment modalities (e.g., self-report, parent, teacher, and clinician rating scales)173, 203, 545 and more objective measurement modalities (e.g., continuous performance task)173 may be sensitive to clinical change in response to treatment, but one study suggested that subjective measures may be more sensitive to detecting treatment-associated changes in ADHD symptom severity and other functional outcomes.203
Three studies assessed the impact on ADHD symptoms of interventions that target medication prescriber training to improve either symptom monitoring or adherence to treatment guidelines. One study assessed the impact of collaborative consultative services,256 and two assessed the impact of a quality improvement intervention on outcome monitoring268, 710 or ADHD symptoms.710 Collectively, the studies showed that medication prescribers (mostly pediatricians) exhibited poor compliance in attending training programs for quality improvement in treating ADHD.256, 268 Even when they did participate in those traininigs, pediatrician compliance with treatment guidelines was poor, as the pediatricians rarely acquired ratings of symptom severity from either parents or, even less often, from teachers,256, 268 even when the intervention increased the collection of ratings compared with waitlist controls.268 Moreover, pediatricians often did not prescribe stimulant medication for youth who met diagnostic criteria for ADHD,255, 256 and when they did prescribe, the doses were sub-optimal,255 even when provided intensive advice and support services from mental health specialists.256 Youth whose prescribers participated in the consultative services from specialists, however, had greater reductions in ADHD symptom severity.256 One study assessed the validity of alerts generated by a computer algorithm based on ratings from monthly monitoring of ADHD symptom severity. Alerts were then sent to prescribers notifying them of putatively actionable clinical events.466 Prescribers deemed the alerts to be generally valid, suggesting that computerized algorithms applied to symptom ratings combined with automated clinican alerts may have clinical utility.
One study of youth who had stimulant-induced weight loss compared the effects of (1) height and weight monitoring alone, with (2) caloric supplementation plus monitoring, and (3) medication holidays plus monitoring on the trajectory of weight gain.274 All three interventions increased weight significantly, suggesting that monitoring of height and weight during medication administration may be efficacious in attenuating stimulant-induced weight loss, though the study did not include the no-intervention control that would have been needed to prove this. Intent-to-treat analyses showed that the addition of caloric supplementation or medication holidays did not provide significant incremental benefit on attenuating weight loss when compared with monitoring alone, though per-protocol analyses suggested that the use of these additional interventions yielded significant additional benefits.
One study used a mobile app to allow patients or their parents to continuously report their clinical status. The study only reported on eight weeks of follow up after initiating the intervention.609 One study continuously assessed patients and evaluated the use of an electronic bottle cap for stimulant medication to monitor treatment adherence.629 Non-adherence was shown to be higher when monitored with this bottle cap compared with patient report, clinician rating, and pill count. The methods used to assess adherence correlated weakly with one another. Non-adherent patients had more severe symptoms at baseline and inferior improvement compared with adherent patients, providing evidence for the validity of the bottle cap method for monitoring adherence. If the bottle cap is considered the gold-standard, then self-reports, clinician impressions, and even pill counts would be deemed unreliable measures of medication adherence.
- Results: Monitoring ADHD - ADHD Diagnosis and Treatment in Children and Adolesce...Results: Monitoring ADHD - ADHD Diagnosis and Treatment in Children and Adolescents
Your browsing activity is empty.
Activity recording is turned off.
See more...